Can a Vertebral Artery Dissection Happen Again
| Vertebral artery dissection | |
|---|---|
| Other names | Vertebral autopsy |
 | |
| Arteries of the neck, with arrows indicating the correct vertebral artery | |
| Specialty | Neurology |
| Symptoms | Headache, difficulty speaking, difficulty swallowing, poor coordination |
| Complications | Stroke, subarachnoid hemorrhage |
| Causes | Trauma, Ehler's Danlos syndrome, Marfan syndrome |
| Diagnostic method | Computed tomography angiography, magnetic resonance angiography, invasive angiography |
| Treatment | Anticoagulation, angioplasty, surgery |
| Medication | Aspirin, heparin, warfarin |
| Frequency | 1.1 per 100,000 |
Vertebral artery dissection (VAD) is a flap-like tear of the inner lining of the vertebral artery, which is located in the neck and supplies blood to the encephalon. After the tear, blood enters the arterial wall and forms a claret clot, thickening the avenue wall and often impeding blood menses. The symptoms of vertebral artery autopsy include head and neck hurting and intermittent or permanent stroke symptoms such as difficulty speaking, impaired coordination and visual loss. It is usually diagnosed with a contrast-enhanced CT or MRI scan.[1] [2]
Vertebral dissection may occur after physical trauma to the neck, such as a blunt injury (e.k. traffic collision), or strangulation, or subsequently sudden neck movements, i.east. cough, but may besides happen spontaneously. 1–4% of spontaneous cases accept a clear underlying connective tissue disorder affecting the blood vessels. Treatment is usually with either antiplatelet drugs such as aspirin or with anticoagulants such as heparin or warfarin.[1]
Vertebral artery dissection is less common than carotid artery dissection (dissection of the big arteries in the front end of the cervix). The two atmospheric condition together account for 10–25% of non-hemorrhagic strokes in young and middle-anile people. Over 75% recover completely or with minimal bear upon on operation, with the remainder having more severe disability and a very modest proportion (most 2%) dying from complications.[ane] [3] It was commencement described in the 1970s by the Canadian neurologist C. Miller Fisher.[three]
Nomenclature [edit]
Vertebral artery dissection is one of the 2 types of dissection of the arteries in the cervix. The other blazon, carotid artery dissection, involves the carotid arteries. Vertebral avenue dissection is further classified equally beingness either traumatic (caused by mechanical trauma to the neck) or spontaneous, and it may also be classified by the part of the artery involved: extracranial (the part exterior the skull) and intracranial (the part within the skull).[1]
Signs and symptoms [edit]
Head pain occurs in 50–75% of all cases of vertebral artery dissection. Information technology tends to be located at the back of the head, either on the affected side or in the eye, and develops gradually. It is either ho-hum or force per unit area-like in character or throbbing. Most half of those with VAD consider the headache singled-out, while the remainder have had a similar headache before.[1] It is suspected that VAD with headache as the only symptom is fairly common;[2] 8% of all cases of vertebral and carotid autopsy are diagnosed on the basis of pain alone.[ane]
Obstruction of blood flow through the affected vessel may lead to dysfunction of part of the brain supplied by the artery. This happens in 77–96% of cases. This may be temporary ("transient ischemic set on") in 10–16% of cases, just many (67–85% of cases) terminate upward with a permanent deficit or a stroke. The vertebral artery supplies the function of the brain that lies in the posterior fossa of the skull, and this type of stroke is therefore chosen a posterior circulation infarct. Problems may include difficulty speaking or swallowing (lateral medullary syndrome); this occurs in less than a 5th of cases and occurs due to dysfunction of the brainstem. Others may experience unsteadiness or lack of coordination due to involvement of the cerebellum, and still others may develop visual loss (on one side of the visual field) due to interest of the visual cortex in the occipital lobe.[1] In the outcome of interest of the sympathetic tracts in the brainstem, a partial Horner'due south syndrome may develop; this is the combination of a drooping eyelid, constricted pupil, and an patently sunken eye on 1 side of the face up.[1]
If the autopsy of the artery extends to the part of the artery that lies inside the skull, subarachnoid hemorrhage may occur (1% of cases). This arises due to rupture of the artery and accumulation of claret in the subarachnoid infinite. It may exist characterized past a dissimilar, unremarkably severe headache; it may also cause a range of additional neurological symptoms.[ane] [ii]
13–16% of all people with vertebral or carotid dissection have dissection in another cervical avenue. It is therefore possible for the symptoms to occur on both sides, or for symptoms of carotid artery dissection to occur at the same time as those of vertebral avenue dissection.[ii] Some give a figure of multiple vessel dissection every bit high as 30%.[three]
Causes [edit]
The causes of vertebral artery dissection can be grouped under 2 main categories, spontaneous and traumatic.
Spontaneous [edit]
Spontaneous cases are considered to be caused by intrinsic factors that weaken the arterial wall.[1] Only a very minor proportion (1–4%) have a articulate underlying connective tissue disorder, such as Ehlers–Danlos syndrome type iv and, more than rarely, Marfan syndrome.[one] [2] All the same, ultrastructural abnormalities of the dermal connective tissue components are discernible in two out of 3 patients with spontaneous dissection.[iv] Ehlers–Danlos syndrome blazon iv, caused by mutations of the COL3A cistron, leads to defective product of the collagen, type 3, alpha 1 poly peptide and causes skin fragility too every bit weakness of the walls of arteries and internal organs.[5] Marfan syndrome results from mutations in the FBN1 cistron, lacking production of the poly peptide fibrillin-1, and a number of physical abnormalities including aneurysm of the aortic root.[v]
In that location have also been reports in other genetic atmospheric condition, such as osteogenesis imperfecta blazon 1, autosomal ascendant polycystic kidney disease and pseudoxanthoma elasticum,[i] α1 antitrypsin deficiency and hereditary hemochromatosis, but bear witness for these associations is weaker.[ii] [vi] Genetic studies in other connective tissue-related genes accept mostly yielded negative results.[ane] Other abnormalities to the blood vessels, such as fibromuscular dysplasia, have been reported in a proportion of cases.[ane] [2] Atherosclerosis does not appear to increment the risk.[1]
There take been numerous reports of associated take a chance factors for vertebral artery dissection; many of these reports suffer from methodological weaknesses, such as selection bias.[7] Elevated homocysteine levels, often due to mutations in the MTHFR gene, appear to increase the chance of vertebral artery dissection.[6] [seven] People with an aneurysm of the aortic root and people with a history of migraine may exist predisposed to vertebral avenue dissection.[7] Vascular tortuosity or redundancy in young patients is associated with an increased run a risk of spontaneous dissection.[8] [9]
Traumatic [edit]
Traumatic vertebral autopsy may follow blunt trauma to the neck, such every bit in a traffic collision, direct blow to the neck, strangulation,[ane] or whiplash injury.[10] 1–2% of those with major trauma may have an injury to the carotid or vertebral arteries.[2] In many cases of vertebral autopsy, people study contempo very mild trauma to the neck or sudden neck movements, e.g. in the context of playing sports. Others report a recent infection, particularly respiratory tract infections associated with coughing.[1] Trauma has been reported to have occurred within a month of dissection in twoscore% with nearly 90% of the traumas existence small-scale.[11] It has been hard to prove the association of vertebral artery autopsy with balmy trauma and infections statistically.[1] Information technology is likely that many "spontaneous" cases may in fact have been caused by such relatively minor insults in someone predisposed by other structural bug to the vessels.[1] A more probable theory, too equally withal unproven, is that the depression-free energy traumatic dissections are actually spontaneous dissections brought to medical attending by the onset of neurological symptoms. These neurological events correspond embolic phenomena due to loosening or breakdown of the clot at the site of the autopsy, which can be triggered by low energy trauma or even occur spontaneously. The fragments travel within the arterial system downstream to the encephalon to cause stroke or stroke-like symptoms.
Vertebral artery dissection has also been reported in association with some forms of cervix manipulation.[12] In that location is meaning controversy most the level of chance of stroke from neck manipulation.[12] It may exist that manipulation can cause dissection,[thirteen] or information technology may be that the autopsy is already present in some people who seek manipulative handling.[xiv] At this fourth dimension, conclusive evidence does not be to support either a strong association betwixt cervix manipulation and stroke, or no clan.[12] Even so, the 2 well-nigh authoritative articles on the subject field, recent literature reviews and analyses, conclude that although in that location exists an association between stroke from vertebral artery dissection and chiropractic adjustment, at that place is bereft show to betoken that the adjustment caused the dissection.[15] [16] A recent meta-assay of the published data on the topic as well looked to apply Colina's criteria for assigning causation in biological systems to the relationship between chiropractic adjustment and cervical artery autopsy, finding that the human relationship did not fulfill the required criteria for causality.[xvi]
Mechanism [edit]
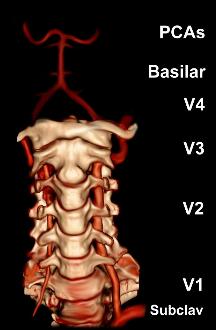
A reconstruction of the vertebral arteries from a CT browse, seen from the front end. From the lesser, V1 is from the subclavian artery to the foramina, V2 is from the foramina to the second vertebra, V3 is between the foramina until entry into the skull, and V4 is inside the skull embedded in the dura mater. They merge into the basilar artery, which then divides into the posterior cerebral artery.
The vertebral arteries arise from the subclavian artery, and run through the transverse foramen of the upper six vertebrae of the cervix. Later on exiting at the level of the kickoff cervical vertebra, its course changes from vertical to horizontal, and so enters the skull through the foramen magnum. Within the skull, the arteries merge to form the basilar artery, which joins the circle of Willis. In total, three quarters of the artery are outside the skull; information technology has a high mobility in this expanse due to rotational movement in the neck and is therefore vulnerable to trauma. Near dissections happen at the level of the first and 2nd vertebrae. The vertebral artery supplies a number of vital structures in the posterior cranial fossa, such equally the brainstem, the cerebellum and the occipital lobes. The brainstem harbors a number of vital functions (such as respiration) and controls the nerves of the face up and neck. The cerebellum is function of the diffuse system that coordinates movement. Finally, the occipital lobes participate in the sense of vision.[1]
Autopsy occurs when blood accumulates in the wall of the claret vessel. This is nearly probable due to a tear in the tunica intima (the inner layer), assuasive claret to enter the tunica media, although other lines of bear witness accept suggested that the claret may instead arise from the vasa vasorum, the modest blood vessels that supply the outer layer of larger blood vessels.[one] [2] Various theories exist as to whether people who sustain carotid and vertebral artery dissection, even if not suffering from a connective tissue disorder, have an underlying vulnerability. Biopsy samples of skin and other arteries has indicated that this might be a possibility, but no genetic defect in collagen or elastin genes has been convincingly proven. Other studies have indicated inflammation of the blood vessels, as measured by highly sensitive C-reactive protein (hsCRP, a marker of inflammation) in the blood.[1]
Once autopsy has occurred, two mechanisms contribute to the evolution of stroke symptoms. Firstly, the menstruation through the blood vessel may be disrupted due to the accumulation of blood under the vessel wall, leading to ischemia (insufficient blood supply). Secondly, irregularities in the vessel wall and turbulence increase the take chances of thrombosis (the formation of claret clots) and embolism (migration) of these clots of the encephalon. From diverse lines of prove, information technology appears that thrombosis and embolism is the predominant trouble.[1]
Subarachnoid hemorrhage due to arterial rupture typically occurs if the dissection extends into the V4 section of the artery. This may exist explained by the fact that the arterial wall is thinner and lacks a number of structural supports in this section.[1] [three] [17]
Diagnosis [edit]

Magnetic resonance angiogram of the neck vessels in a person with Ehlers-Danlos syndrome type IV; it shows a dissection of the left internal carotid artery, dissection of both vertebral arteries in their V1 and V2 segments and a dissection of the heart and distal 3rd of the correct subclavian artery. Such striking episodes of dissection are typical for this "vascular" subtype of Ehlers-Danlos syndrome.
Various diagnostic modalities exist to demonstrate blood menstruum or absenteeism thereof in the vertebral arteries. The gold standard is cognitive angiography (with or without digital subtraction angiography).[3] [eighteen] [nineteen] This involves puncture of a large avenue (usually the femoral artery) and advancing an intravascular catheter through the aorta towards the vertebral arteries. At that betoken, radiocontrast is injected and its downstream catamenia captured on fluoroscopy (continuous Ten-ray imaging).[20] The vessel may appear stenotic (narrowed, 41–75%), occluded (blocked, 18–49%), or as an aneurysm (expanse of dilation, v–xiii%). The narrowing may exist described as "rat'south tail" or "string sign".[1] Cerebral angiography is an invasive procedure, and it requires large volumes of radiocontrast that can cause complications such as kidney damage.[20] Angiography besides does not directly demonstrate the blood in the vessel wall, as opposed to more than modern modalities.[ane] [2] The simply remaining use of angiography is when endovascular treatment is contemplated (see below).[one]
More modern methods involve computed tomography (CT angiography) and magnetic resonance imaging (MR angiography). They use smaller amounts of dissimilarity and are non invasive. CT angiography and MR angiography are more or less equivalent when used to diagnose or exclude vertebral artery autopsy.[xviii] CTA has the advantage of showing certain abnormalities earlier, tends to be available outside office hours, and can be performed speedily.[i] When MR angiography is used, the best results are achieved in the T1 setting[2] using a protocol known equally "fat suppression".[1] [2] [3] Doppler ultrasound is less useful equally it provides little information about the office of the artery close to the skull base and in the vertebral foramina, and any abnormality detected on ultrasound would still require confirmation with CT or MRI.[1] [ii] [3]
Treatment [edit]
Treatment is focused on reducing stroke episodes and damage from a distending artery.[3] Four treatment modalities have been reported in the treatment of vertebral artery dissection. The two chief treatments involve medication: anticoagulation (using heparin and warfarin) and antiplatelet drugs (usually aspirin). More than rarely, thrombolysis (medication that dissolves blood clots) may be administered, and occasionally obstruction may be treated with angioplasty and stenting. No randomized controlled trials have been performed to compare the different handling modalities.[ane] [21] Surgery is only used in infrequent cases.[1]
Anticoagulation and aspirin [edit]

Aspirin (tablets pictured) is commonly used subsequently stroke. In vertebral artery dissection it appears every bit constructive every bit anticoagulation with warfarin.
From analysis of the existing small treatment trials of cervical artery dissection (carotid and vertebral) information technology appears that aspirin and anticoagulation (heparin followed by warfarin) are equally effective in reducing the take a chance of further stroke or death. Anticoagulation is regarded as more powerful than antiplatelet therapy, but anticoagulants may increase the size of the hematoma and worsen obstruction of the affected avenue.[21] Anticoagulation may be relatively unsafe if a large stroke has already occurred, as hemorrhagic transformation is relatively common, and if the dissection extends into V4 (conveying a risk of subarachnoid hemorrhage). Anticoagulation may be appropriate if there is rapid blood flow (through a severely narrowed vessel) on transcranial doppler despite the use of aspirin, if in that location is a completely occluded vessel, if there are recurrent stroke-like episodes, or if free-floating blood clot is visible on scans.[1] [ii] [22] Warfarin is typically continued for 3–6 months, as during this time the flow through the artery usually improves, and most strokes happen inside the offset 6 months after the development of the autopsy.[1] Some regard 3 months as sufficient.[3]
Professional guidelines in the UK recommend that patients with VA autopsy should be enrolled in a clinical trial comparison aspirin and anticoagulation if possible.[23] American guidelines state that the benefit of anticoagulation is not currently established.[24]
Thrombolysis, stenting and surgery [edit]
Thrombolysis, stenting and surgery are not used as widely equally anticoagulation or antiplatelet drugs. These treatments are invasive, and are typically reserved for situations where symptoms worsen despite medical treatment, or where medical treatment may be unsafe (e.chiliad. an unacceptable bleeding tendency).[i] [2]
Thrombolysis is enzymatic destruction of blood clots. This is achieved by the administration of a drug (such equally urokinase or alteplase) that activates plasmin, an enzyme that occurs naturally in the body and digests clots when activated. Thrombolysis is an accustomed treatment for middle attacks and stroke unrelated to dissection. In cervical artery dissection, simply modest example series are bachelor. The thrombolytic drug is administered either intravenously or during cerebral angiography through a catheter directly into the afflicted avenue. The data indicates that thrombolysis is safe, but its place in the handling of VAD is uncertain.[21]
Stenting involves the catheterization of the affected artery during angiography, and the insertion of a mesh-like tube; this is known as "endovascular therapy" (inside the blood vessel). This may be performed to allow the blood to menstruation through a severely narrowed vessel, or to seal off an aneurysm. However, information technology is unclear whether the technical success of the procedure translates into improved outcomes, as in both cases the trouble often resolves spontaneously over time.[21] Stenting, as well as the insertion of coils by means of angiography, may be performed if there is an aneurysm and/or extension of the dissection into the V4 section of the artery.[17]
Surgery carries a high run a risk of complications, and is typically simply offered in case of inexorable deterioration or contraindications to any of the other treatments. Various arterial repair procedures have been described.[1] [17]
Prognosis [edit]
Prognosis of spontaneous cervical arterial autopsy involves neurological and arterial results. The overall functional prognosis of individuals with stroke due to cervical artery dissection does non announced to vary from that of young people with stroke due to other causes. The charge per unit of survival with skillful outcome (a modified Rankin score of 0–2) is generally nigh 75%,[one] [3] or perhaps slightly better (85.7%) if antiplatelet drugs are used.[ane] In studies of anticoagulants and aspirin, the combined mortality with either treatment is one.8–2.i%.[ane] [21]
Afterward the initial episode, ii% may experience a farther episode within the get-go month. After this, at that place is a 1% annual hazard of recurrence.[1] Those with high blood pressure and dissections in multiple arteries may take a higher risk of recurrence.[two] Further episodes of cervical avenue dissection are more common in those who are younger, have a family history of cervical artery dissection, or accept a diagnosis of Ehlers-Danlos syndrome or fibromuscular dysplasia.[two]
Epidemiology [edit]
The annual incidence is most ane.1 per 100,000 annually in population studies from the United states of america and French republic. From 1994 to 2003, the incidence increased threefold; this has been attributed to the more widespread use of modern imaging modalities rather than a true increment.[1] Similarly, those living in urban areas are more probable to receive appropriate investigations, bookkeeping for increased rates of diagnosis in those dwelling in cities. Information technology is suspected that a proportion of cases in people with mild symptoms remains undiagnosed.[ii]
In that location is controversy as to whether VAD is more common in men or in women; an aggregate of all studies shows that it is slightly higher incidence in men (56% versus 44%).[ane] Men are on average 37–44 years old at diagnosis, and women 34–44. While autopsy of the carotid and vertebral arteries accounts for only 2% of strokes (which are usually caused past loftier claret pressure and other risk factors, and tend to occur in the elderly), they crusade 10–25% of strokes in young and middle-anile people.[1] [3]
Dissecting aneurysms of the vertebral artery constitute 4% of all cognitive aneurysms, and are hence a relatively rare but of import cause of subarachnoid hemorrhage.[17]
History [edit]
Spontaneous vertebral avenue dissection was described in the 1970s. Prior to this, there had been isolated example reports about carotid autopsy. In 1971, C. Miller Fisher, a Canadian neurologist and stroke physician working at Massachusetts General Hospital, beginning noted the "string sign" abnormality in carotid arteries on cerebral angiograms of stroke patients, and later on discovered that the aforementioned abnormality could occur in the vertebral arteries. He reported the discovery in a paper in 1978.[3] [25] [26]
Notable cases [edit]
Australian cricketer Phillip Hughes died on 27 November 2022 after developing a vertebral artery dissection as a consequence of existence struck on the side of the cervix by a cricket brawl during a Sheffield Shield match on 25 November 2014. The ball struck Hughes on the base of the skull just behind his left ear which caused a vertebral avenue dissection complicated by subarachnoid hemorrhage.[27]
References [edit]
- ^ a b c d eastward f 1000 h i j k 50 thousand n o p q r south t u five w ten y z aa ab ac ad ae af ag ah ai aj ak al am an ao ap aq Kim YK, Schulman South (April 2009). "Cervical artery autopsy: pathology, epidemiology and management". Thromb. Res. 123 (six): 810–21. doi:10.1016/j.thromres.2009.01.013. PMID 19269682.
- ^ a b c d e f chiliad h i j k l m due north o p q r Debette S, Leys D (July 2009). "Cervical-artery dissections: predisposing factors, diagnosis, and upshot". Lancet Neurol. 8 (seven): 668–78. doi:10.1016/S1474-4422(09)70084-v. PMID 19539238.
- ^ a b c d east f 1000 h i j k l Campos-Herrera CR, Scaff M, Yamamoto FI, Conforto AB (December 2008). "Spontaneous cervical artery dissection: an update on clinical and diagnostic aspects". Arq Neuropsiquiatr. 66 (4): 922–seven. doi:10.1590/S0004-282X2008000600036. PMID 19099146.
- ^ Schievink, Wouter I. (2001-03-22). "Spontaneous Autopsy of the Carotid and Vertebral Arteries". New England Periodical of Medicine. 344 (12): 898–906. doi:10.1056/NEJM200103223441206. ISSN 0028-4793.
- ^ a b Callewaert B, Malfait F, Loeys B, De Paepe A (March 2008). "Ehlers-Danlos syndromes and Marfan syndrome". Best Pract Res Clin Rheumatol. 22 (1): 165–89. doi:10.1016/j.berh.2007.12.005. PMID 18328988.
- ^ a b Debette Southward, Markus HS (June 2009). "The genetics of cervical artery autopsy: a systematic review". Stroke. 40 (6): e459–66. doi:10.1161/STROKEAHA.108.534669. PMID 19390073.
- ^ a b c Rubinstein SM, Peerdeman SM, van Tulder MW, Riphagen I, Haldeman South (July 2005). "A systematic review of the risk factors for cervical artery autopsy". Stroke. 36 (vii): 1575–lxxx. doi:10.1161/01.STR.0000169919.73219.30. PMID 15933263.
- ^ Kim, Bum Joon; Yang, Ewha; Kim, Na-Young; Kim, Mi-Jung; Kang, Dong-Wha; Kwon, Sun U.; Kim, Jong Due south. (October 2016). "Vascular Tortuosity May Exist Associated With Cervical Artery Dissection". Stroke. 47 (x): 2548–2552. doi:ten.1161/STROKEAHA.116.013736. ISSN 0039-2499.
- ^ Barbour, P J; Castaldo, J Eastward; Rae-Grant, A D; Gee, Due west; Reed, J F; Jenny, D; Longennecker, J (June 1994). "Internal carotid artery back-up is significantly associated with dissection". Stroke. 25 (six): 1201–1206. doi:10.1161/01.STR.25.6.1201. ISSN 0039-2499.
- ^ Siegmund, GP; Winkelstein, BA; Ivancic, PC; Svensson, MY; Vasavada, A (April 2009). "The anatomy and biomechanics of acute and chronic whiplash injury". Traffic Injury Prevention. 10 (2): 101–12. doi:x.1080/15389580802593269. PMID 19333822.
- ^ Debette, Southward (February 2014). "Pathophysiology and risk factors of cervical avenue autopsy: what have we learnt from large hospital-based cohorts?". Electric current Opinion in Neurology. 27 (1): 20–8. doi:x.1097/wco.0000000000000056. PMID 24300790.
- ^ a b c Haynes MJ, Vincent K, Fischhoff C, Bremner AP, Lanlo O, Hankey GJ (2012). "Assessing the risk of stroke from cervix manipulation: a systematic review". International Journal of Clinical Exercise. 66 (10): 940–947. doi:10.1111/j.1742-1241.2012.03004.ten. PMC3506737. PMID 22994328.
- ^ Ernst Due east (2010). "Vascular accidents after neck manipulation: cause or coincidence?". Int J Clin Pract. 64 (6): 673–7. doi:10.1111/j.1742-1241.2009.02237.x. PMID 20518945.
- ^ Guzman J, Haldeman S, Carroll LJ, et al. (February 2009). "Clinical practice implications of the bone and joint decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders: from concepts and findings to recommendations". J Manipulative Physiol Ther. 32 (2 Suppl): S227–43. doi:x.1016/j.jmpt.2008.eleven.023. PMID 19251069.
In persons younger than 45 years, at that place is an association between chiropractic care and vertebro-basilar artery (VBA) stroke; there is a like association between family physician care and VBA stroke. This suggests that in that location is no increased adventure of VBA stroke after chiropractic care, and that these associations are likely due to patients with headache and cervix hurting from vertebral artery dissection seeking care while in the prodromal phase of a VBA stroke. Unfortunately, there is no practical or proven method to screen patients with cervix hurting and headache for vertebral artery autopsy. Withal, VBA strokes are extremely rare, especially in younger persons.
- ^ Biller, José; Sacco, Ralph L.; Albuquerque, Felipe C.; Demaerschalk, Bart G.; Fayad, Pierre; Long, Preston H.; Noorollah, Lori D.; Panagos, Peter D.; Schievink, Wouter I.; Schwartz, Neil E.; Shuaib, Ashfaq (October 2014). "Cervical Arterial Dissections and Association With Cervical Manipulative Therapy: A Argument for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke. 45 (10): 3155–3174. doi:x.1161/STR.0000000000000016. ISSN 0039-2499.
- ^ a b Church, Ephraim W; Sieg, Emily P; Zalatimo, Omar; Hussain, Namath Due south; Glantz, Michael; Harbaugh, Robert E (2016-02-16). "Systematic Review and Meta-analysis of Chiropractic Care and Cervical Avenue Dissection: No Evidence for Causation". Cureus. doi:10.7759/cureus.498. ISSN 2168-8184. PMC4794386. PMID 27014532.
- ^ a b c d Santos-Franco JA, Zenteno G, Lee A (April 2008). "Dissecting aneurysms of the vertebrobasilar arrangement. A comprehensive review on natural history and handling options". Neurosurg Rev. 31 (2): 131–twoscore, give-and-take 140. doi:x.1007/s10143-008-0124-x. PMID 18309525.
- ^ a b Provenzale JM, Sarikaya B (October 2009). "Comparison of exam performance characteristics of MRI, MR angiography, and CT angiography in the diagnosis of carotid and vertebral artery dissection: a review of the medical literature". AJR Am J Roentgenol. 193 (4): 1167–74. doi:10.2214/AJR.08.1688. PMID 19770343.
- ^ Latchaw RE, Alberts MJ, Lev MH, et al. (November 2009). "Recommendations for imaging of astute ischemic stroke: a scientific statement from the American Middle Association". Stroke. xl (eleven): 3646–78. doi:10.1161/STROKEAHA.108.192616. PMID 19797189.
- ^ a b Kaufmann TJ, Kallmes DF (June 2008). "Diagnostic cognitive angiography: archaic and complication-prone or here to stay for another 80 years?". AJR Am J Roentgenol. 190 (vi): 1435–7. doi:10.2214/AJR.07.3522. PMID 18492888.
- ^ a b c d eastward Menon R, Kerry S, Norris JW, Markus HS (October 2008). "Handling of cervical artery autopsy: a systematic review and meta-analysis". J. Neurol. Neurosurg. Psychiatry. 79 (10): 1122–7. doi:10.1136/jnnp.2007.138800. PMID 18303104.
- ^ Engelter ST, Brandt T, Debette Due south, et al. (September 2007). "Antiplatelets versus anticoagulation in cervical artery dissection". Stroke. 38 (nine): 2605–11. doi:10.1161/STROKEAHA.107.489666. PMID 17656656.
- ^ National Establish for Health and Clinical Excellence. Clinical guideline 68: Stroke. London, 2008.
- ^ Adams HP, del Zoppo G, Alberts MJ, et al. (May 2007). "Guidelines for the early on management of adults with ischemic stroke". Stroke. 38 (5): 1655–711. doi:ten.1161/STROKEAHA.107.181486. PMID 17431204.
- ^ Fisher CM, Ojemann RG, Roberson GH (February 1978). "Spontaneous dissection of cervico-cerebral arteries". Tin J Neurol Sci. five (i): 9–xix. doi:10.1017/S0317167100024690. PMID 647502.
- ^ Fisher CM (November 2001). "A career in cerebrovascular affliction: a personal account". Stroke. 32 (11): 2719–24. doi:ten.1161/hs1101.098765. PMID 11692045.
- ^ Coverdale, Brydon (27 November 2014). "Hughes suffered extremely rare, freak injury to neck". ESPN. Retrieved 27 November 2014.
External links [edit]
- Cervical Artery Dissections and Ischemic Stroke Patients, international research collaboration into cervical artery autopsy
Encounter also [edit]
- Aortic dissection
- Carotid artery dissection
Source: https://en.wikipedia.org/wiki/Vertebral_artery_dissection#:~:text=After%20the%20initial%20episode%2C%202,a%20higher%20risk%20of%20recurrence.
0 Response to "Can a Vertebral Artery Dissection Happen Again"
Post a Comment